Biopsy
Definition
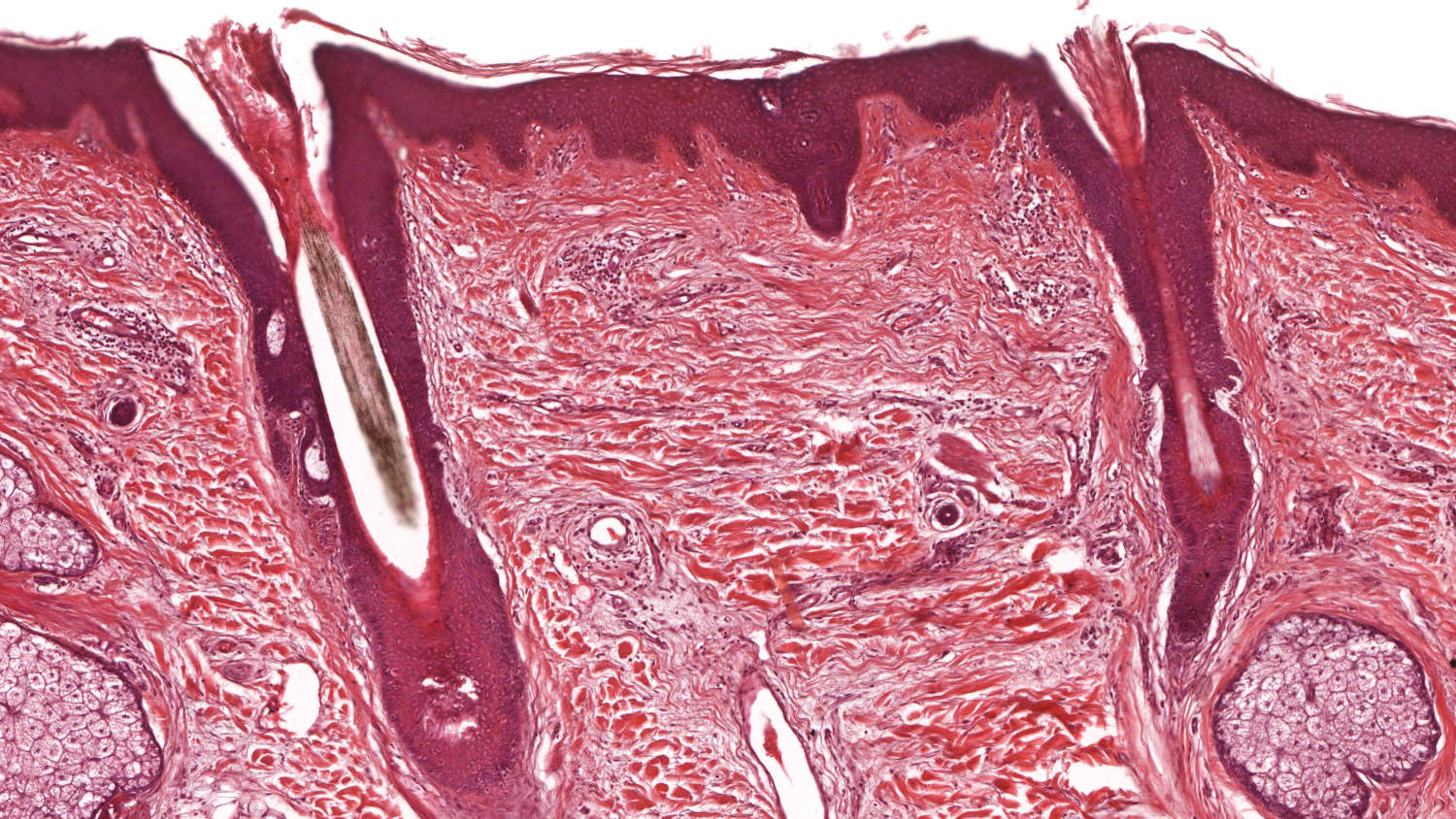
A biopsy is a medical procedure in which a small sample of tissue is removed from a specific area of the body for examination under a microscope. This diagnostic technique helps doctors determine the presence, cause, or extent of a disease, such as cancer or infection.